Secretary of Veterans Affairs Doug Collins testifies during a House Committee on Appropriations subcommittee budget hearing on Capitol Hill, Thursday, May 15, 2025, in Washington. (Yuri Gripas, AP Photo)
James Jones is a 54-year-old disabled Army veteran. After four years of active duty—some of it in the Gulf War—and four years in the reserves, Jones says he has a “multitude” of health care problems.
Ask him to list his health care needs and he sighs and reels off a long list. “Oh my, I have a multitude of stuff. There’s PTSD [post-traumatic stress disorder], a right arm injury, my right shoulder, chronic rhinitis from toxic exposure during the Gulf War, dental. It all adds up,” he says, laughing, “to a 100% disability rating in VA math.” That’s why he depends on the services provided by the health care system—the nation’s largest—run by the Department of Veterans Affairs (VA).
Secretary of Veterans Affairs Doug Collins testifies during a House Committee on Appropriations subcommittee budget hearing on Capitol Hill, Thursday, May 15, 2025, in Washington. (Yuri Gripas, AP Photo)
Jones is also one of the hundreds of thousands of disabled veterans who work for the federal government, in his case the National Park Service. Plus, he’s one of the 25% of vets who live in a rural area like Wakauga County, North Carolina.
“I’m an hour’s drive away from the VA outpatient clinic in Hickory,” he says, “and a two-hour drive from the VA hospital in Asheville.”
On the face of it, Jones would seem to be a poster boy for the kind of private sector health care so many Republicans, including Donald Trump and his VA Secretary former Georgia Congressman Doug Collins, want to see replace the VA.
For over a decade, Republicans in Congress—with the acquiescence of many Democrats—have passed legislation to outsource the care provided to nine million veterans. The main vehicle for this shift was one of the only legislative wins of the first Trump administration: the VA MISSION Act of 2018.
MISSION (a doublespeak acronym the bill’s authors coined for “maintaining internal systems and strengthening integrated outside networks”) established a parallel private network, the Veterans Community Care Program (VCCP), which now sees 60% of VA patients and contracts with over 1.7 million doctors, therapists, hospitals and other private providers. Each year the VCCP eats up more funding. It’s now consuming over $30 billion a year that could go to hiring more staff and improving the VA’s aging infrastructure. This year, as part of the annual appropriations bill for the VA, Doug Collins, who was appointed by Trump in February to lead the VA, asked Congress for a 50% increase in discretionary funding for the VCCP and, in an unprecedented move, asked to reduce VA funding by 17%.
Collins’s proposal passed in June along party lines in the House, and in August passed the Senate with an overwhelming bipartisan majority (9 senators voted against it). In his testimony before the Senate in June, Collins’s insisted that his policies were not “cutting benefits and health care,” but instead “making sure Veterans were getting the health care choices they were promised under the Maintaining Internal Systems and Strengthening Integrated Outside Networks Act.” In fact, Collins proposals and his budget priorities make clear that he is interested only in strengthening outside networks rather than maintaining internal systems.
Proponents of this version of privatization insist their policies support rural veterans like James Jones. Jon Tester, a former Senator from Montana and Democratic architect of the MISSION Act, argued—as other VA privatizers in Congress continue to do—that rural vets are forced to drive too far and wait too long for a VA appointment. The private sector, they insist, can provide rural veterans with high quality, conveniently located care without the kinds of delays they may face at the VA.
James Jones, an Army veteran, is one of 4.7 million veterans who live in rural America. He is wary of efforts to divert funding away from the VA system to non-VA private providers. (James Jones)
James Jones and many other rural veterans say this is a big lie. “I prefer to go to the VA, even if I have to drive longer to get there,” he says. But even if he wanted to take advantage of non-VA providers, the fact is there are simply not enough in Boone or anywhere else in rural America to accommodate the needs and absorb the influx of the 4.7 million rural veterans like himself.
That’s precisely what the Veterans Healthcare Policy Institute (VHPI) found when it analyzed private sector health care capacity in all 50 states. In a study entitled “Veterans Healthcare Choice—Myth or Reality? A State-By-State Reality Check of the False Promise of VA Privatization,” VHPI discovered that rural veterans seeking care in the private sector face even greater barriers to accessing health care, as they encounter the same long-standing rural health care crisis that prevents their loved ones, friends and neighbors from receiving needed care. (Editor’s note: Suzanne Gordon, one of the present authors, was the main author of that report.)
Consider the facts.
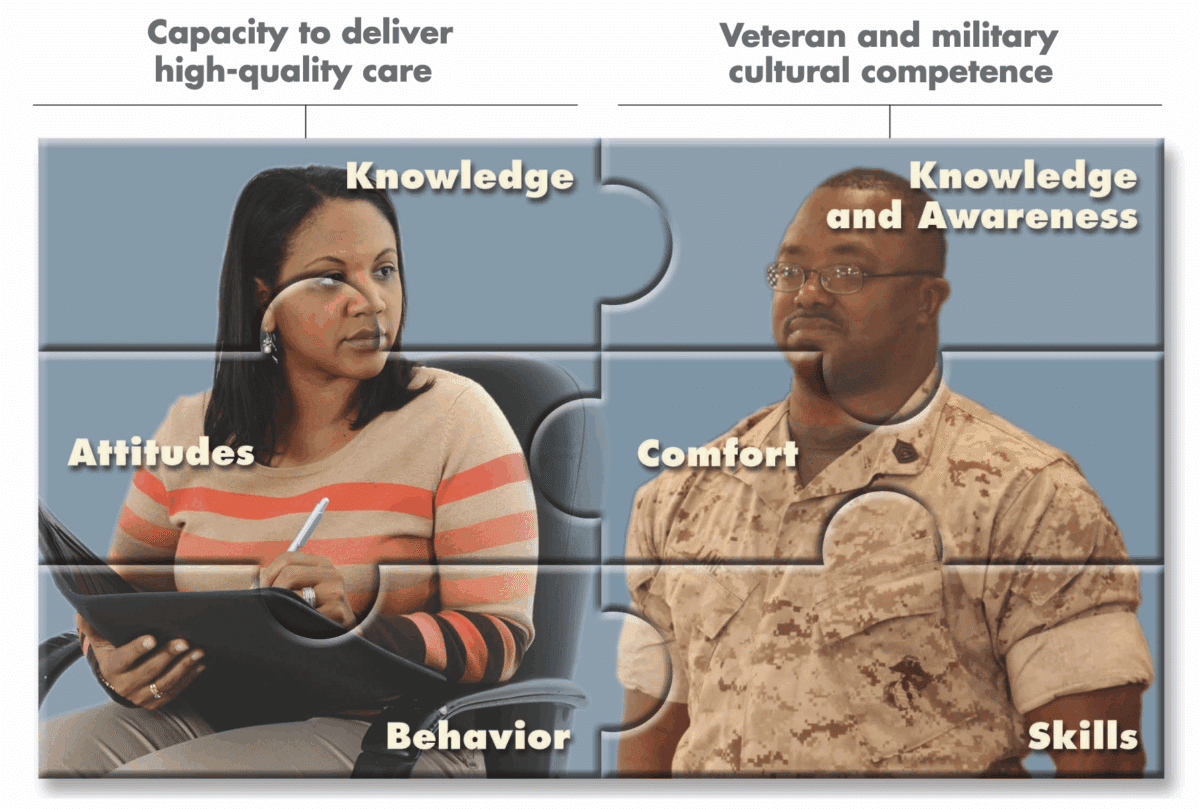
Many lawmakers representing rural America, like Republican Sens. Jerry Moran of Kansas, Marsha Blackburn of Tennessee and Bill Cassidy of Louisiana (all of whom sit on the Senate Committee on Veterans Affairs) insist that private sector health care providers are not only willing but able to provide high quality care to veterans. While these providers may be well-intentioned, and eager to help veterans, few of them have enough knowledge or expertise to recognize veterans’ complex health care problems, much less treat them. This was the conclusion of not one but two RAND Corporation studies of private sector providers.
In a 2014 study “Ready to Serve,” which looked at competence to treat the over 41% of vets with mental health problems, RAND found that only 8% of private providers understood military culture—compared to 70% in the VA. Moreover, 18% of respondents “agreed that diagnosing and treating military personnel and veterans with mental health problems is no different than diagnosing and treating civilians with mental health problems.” For those who know how hard it is to treat vets with severe combat related PTSD that’s a truly shocking assumption.
“Readiness for Veteran-Friendly, High-Quality Mental Health Care,” an image from a 2014 RAND Corporation study looking at the capacity of mental health providers in treating veterans. (RAND Corporation)
Four years later, in 2018, RAND conducted a similar study, of primary care and mental health providers in the state of New York aptly titled “Ready or Not,” and found similar results. Most providers did not even know if their patients were veterans and didn’t bother to ask. Many were unfamiliar with evidence- based treatments for common military related mental health conditions. The report concluded, “While 92 percent of New York health care providers were accepting new patients, only 2.3 percent met all criteria for effectively serving the veteran population.”
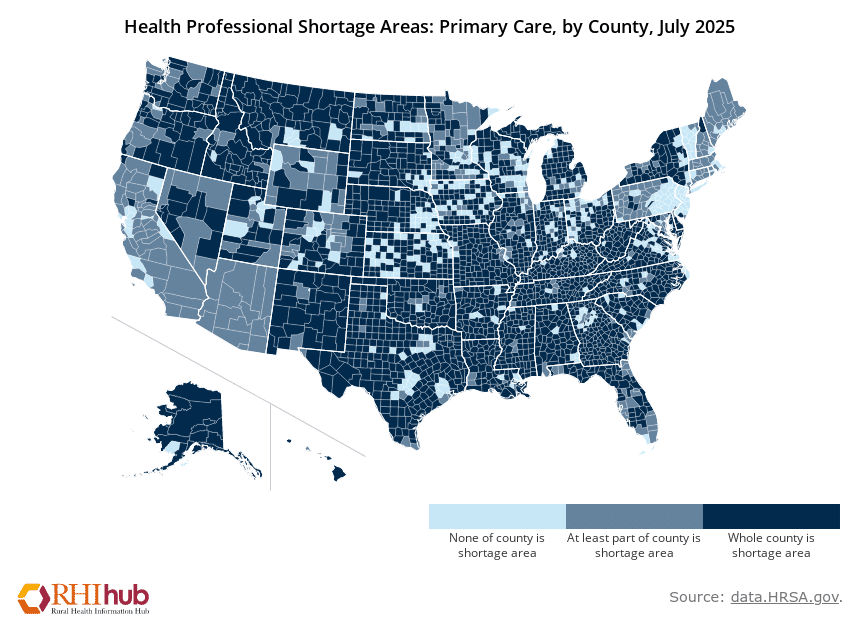
For rural veterans the problem isn’t just finding a provider who understands their complex health conditions—it’s finding any provider at all. That’s because the majority of rural Americans live in so-called medical and mental health deserts that. In the United States, 89% of counties are officially designated Health Professional Shortage Areas (HPSAs) for primary care, based on a range of medical, economic and geographic vulnerabilities identified by the U.S. Department of Health and Human Services. For example, 79 million Americans (that’s 23% of the U.S. population and 30% of the adult population) live in areas with shortages of primary care providers. In states with large rural populations like Georgia, North Carolina and Texas, nearly every rural county, and many urban ones, fall under this designation.
Map showing county-level data on Primary Care Health Professional Shortage Areas (HPSAs), indicating counties that are entirely in a HPSA, partially in a HPSA, or not in a HPSA. (Health Resources & Services Administration)
When it comes to the ability to find a psychologist, psychiatrist or social worker, 123 million people—that’s over one-third of the country’s population and almost half of the adult population—live in a Mental Health Professional Shortage Area (MHPSA). Among rural counties, 81% do not have a single psychiatric nurse practitioner and 65% do not have a single psychiatrist. This huge gap particularly affects veterans in rural areas, as more than 41% of veterans are dealing with mental health conditions.
Bob Anderson, a Vietnam veteran who lives in Albuquerque, New Mexico, can recount the many ways private sector providers have let him down. (Courtesy of Bob Anderson)
Bob Anderson, an 81-year-old Vietnam veteran, who lives in Albuquerque, New Mexico, has been very frustrated with the kind of experiences he has had with private sector providers:
I’ve been sent to community care for dental and periodontal treatment and when I had to have a pretty extensive basal cell carcinoma removed from my upper lip. When I went to the private sector cancer doctor, my appointment was late in the afternoon on a Friday, and they prescribed pain meds that I had to pick up at the VA which was all the way across town. It was very difficult to get the pain medicine I needed.
Doctors, Anderson adds, also had no information about what medication he was taking, which can be very important for a man with a heart condition who is having either dental or other surgeries. Plus, Anderson says, there was no effort to coordinate or follow up his care.
In his 35 years of being part of the VA system, Anderson says:
You’d always get a call from a nurse or nurse practitioner the next day to see how you were doing. One nurse practitioner from my primary care provider at the VA would call me and talk to me for about a half an hour to make sure I was doing everything I was supposed to be doing. Although I sometimes thought it was a bit much, she was really very good. Never have I gotten a call at all from any of the community providers I’ve gone to.
If rural veterans need hospital care for an emergency, to deliver a baby or get chemotherapy, they will have a hard time finding one that hasn’t closed or eliminated services. Of the less than 1,800 rural hospitals remaining, “2025 Rural Health State of the State,” a report by the health care consulting company Chartis, found that 432 rural hospitals are “vulnerable to closure,” with 46% having a negative operating margin.
Over the past 15 years, Chartis explains, 182 rural hospitals, have either closed or no longer provide inpatient care. Between 2014 and 2023, 424 stopped delivering chemotherapy for patients with cancer.
A July 2025 article in Health Affairs highlighted the dramatic decline in hospitals providing obstetrical services across the nation. Not surprisingly, this service cut is more acute in rural areas, with “twelve states (25.5 percent) experiencing 25 percent or more losses of obstetric services among hospitals in rural counties.”
The loss of obstetrical services has serious implications for women veterans who are the fastest growing group in the veteran population.
These statistics, which paint a bleak picture of the rural health care landscape, pre-date the passage of President Trump’s new budget, which will decimate rural hospitals and discourage even more medical and mental health professionals from practicing in rural areas. If nine million veterans are steered into crumbling rural health care institutions and practices, rather than relying on the VA, a specialized system designed to care for their specific needs, veterans will be forced to compete with their loved ones, friends and community members for increasingly scarce rural health care resources.
Fortunately, huge opposition is forming all over the country to the administration’s VA priorities and other efforts to dismantle the federal government. James Jones is part of that opposition. What he and his fellow veterans want is not more costly and unnecessary outsourcing but improvements in the VA.
Suzanne Gordon is a journalist, author, and editor, who has written extensively about health care work and policy issues. She has published three books about the veterans’ healthcare system, including most recently Our Veterans: Winners, Losers, Friends and Enemies on the New Terrain of Veterans Affairs from Duke University Press (co-authored with Steve Early and Jasper Craven). Her work has appeared in the New York Times, Boston Globe, American Prospect, The Nation, Jacobin, Atlantic Monthly, and many other publications. She also lives in Richmond and works with the Bay Area-based Veterans Healthcare Policy Institute. She can be contacted via her website, suzannegordon.com.
Steve Early has been writing about politics or labor in Vermont since he was an undergraduate at Middlebury College more than fifty years ago. He is a former international union representative for the Communications Workers of America and was involved in organizing, bargaining, and political action by CWA members and other workers throughout New England. He co-founded “Labor for Bernie” and was active in both Sanders for President campaigns. Since moving to the Bay Area, he authored four books, including Refinery Town: Big Oil, Big Money, and the Remaking of an American City (Beacon Press) about his new hometown, Richmond, California. He can be reached at Lsupport@aol.com.
Have thoughts or reactions to this or any other piece that you’d like to share? Send us a note with the Letter to the Editor form.